

Abstract
Introduction:
Hospitalization-associated VTE attack (incident plus recurrent VTE) rates over the 6-year period, 2005-2010, did not change significantly despite achieving near-universal in-hospital VTE prophylaxis; 75% of these VTE events occurred after hospital discharge with a median of 19.5 days from hospital discharge to VTE. The median durations of hospitalization and in-hospital prophylaxis were 3 days and 70 hours, respectively, suggesting that VTE prophylaxis was inadequate. However, the hospital population that would benefit most from post-hospitalization VTE prophylaxis is uncertain. Our study aim was to test hospital length of stay (LOS) as a potential predictor of post-hospital-discharge incident or recurrent VTE.
Methods:
Using the resources of the Rochester Epidemiology Project, we identified all unique Olmsted County, MN residents hospitalized at least once at a Rochester, MN Mayo Clinic hospital and all such residents with objectively-diagnosed occurrence of first or recurrent VTE during hospitalization or within 92 days after hospital discharge, 2005-2010. We tested LOS as a potential predictor of post-hospital-discharge VTE (conditional on surviving to hospital discharge free of VTE) using the Anderson-Gill version of Cox regression modeling and adjusting for age, sex, any surgery performed during that hospitalization, and Charlson Comorbidity Index calculated from conditions recorded from 1/1/2005 until the day of hospital discharge.
Results:
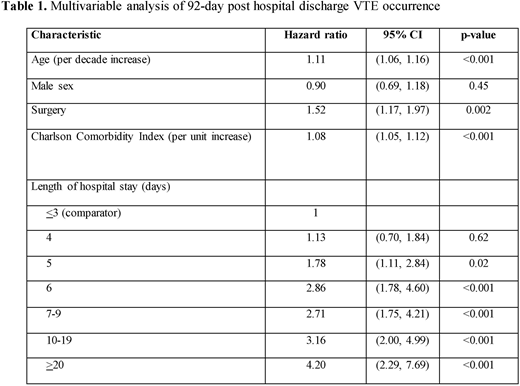
Over the period, 2005-2010, 31,588 unique Olmsted County residents were hospitalized at least once at a Rochester Mayo Clinic hospital. The distribution of LOS was: 1-2 (3.8%), 3 (24.2%), 4 (23.3%), 5 (16.4%), 6 (8.8%), 7-9 (12.4%), 10-19 (8.4%) and 20+ (2.3%). Of the 253 VTE events identified within 92 days post-hospital discharge, 6, 29, 31, 38, 38, 53, 42 and 16 had been hospitalized for 1-2, 3, 4, 5, 6, 7-9, 10-19 and 20+ days, respectively. The hazard ratios (HR) for post-hospital-discharge VTE were similar for hospital LOS ≤4 days; compared to LOS ≤3 days, the HRs were significantly increased for hospital LOS of 5 (HR=1.78), 6 (HR=2.86), 7-9 (HR=2.71), 10-19 (HR=3.16) and 20+ (HR=4.20) days (Table 1).
Conclusions:
The adjusted hazards of post-hospital discharge VTE for hospital LOS > 4 days were significantly increased 1.8 to 4.2-fold compared to LOS ≤3 days, suggesting that hospital LOS may be useful for identifying hospitalized patients suitable for longer duration VTE (including post-discharge) prophylaxis. Future studies should be aimed at identifying additional predictors of post-hospital-discharge VTE such that extended prophylaxis can be targeted to those patients who would benefit most.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal